Autism Treatments Rationale
Among several known autism treatments claiming to help autistic child to communicate and perform better, to feel less frustrated and even happier, there is no miracle therapy which totally cures autism. However with some of them significant improvements have been noted especially in improving adaptive behaviour and learning potential. For parents striving to help their autistic child, one of the crucial questions is what is the correct course of actions to take? Which treatment out of several existing autism treatments to start with?

Guy Richards from Perry Baromedical in his Discussion Paper "The Autistic Child and Options for Treatment" offers a discussion about a rational behind several known autism treatments based upon the various hypotheses for autism causes in order to improve the understanding of parents and stimulate debate amongst medical practitioners.
Following are the brief facts from Guy Richards' background: Guy Richards, MA CChem, MRSC (Master of Arts, Chartered Chemist, is a Member of the Royal Society of Chemistry). MA in Natural Sciences, Chemistry and Chemical Pharmacology, Oxford University. Thesis: The Preparation & Properties of Some Irreversible Inhibitors of Acetyl Cholinesterase. 13 Years Group Manager R&D Pharmaceuticals & Intermediates Courtaulds Chemicals. Member ASME PVHO Committee & Sub-committees since 2003. Technical Director Blanson manufacturer of Acrylic Pressure Windows for HBOT, biopharmaceutical purifications & submersibles. Currently Guy is a Technology Transfer Manager, Perry Baromedical European Office.
The Autistic Child and Options for Treatment
A Discussion Paper
By Guy Richards
Aim
The aim of this Discussion Paper is to offer an autism treatments rationale for autistic children based upon the various hypotheses for its causation in order to help improve the understanding of parents and stimulate debate amongst medical practitioners. The author has applied a Most Probable Cause Analysis based upon Kepner-Tregoe methodologies to the latest publications available. The opinions expressed are the authors own and it must be stressed that parents of autistic children should seek guidance from a trusted medical practitioner before adopting any treatments discussed in this Paper.
Background
Autism is a broad spectrum catch-all description of children with a diverse range of developmental problems and social skills which prevent them interacting in a positive or loving manner as well as a number of associated conditions such as digestive disorders.
As many as 1 in 166 children in the USA are diagnosed with one category or other of this distressing condition; covering qualitative abnormalities in social interactions, marked by very poor communication skills, and by habitual repetitive and stereotypical behaviours. Some authorities put this figure as high as 1 in 91 although there are some concerns about over-diagnosis. (Max Wiznitzer, MD, of Rainbow Babies & Childrens Hospital in Cleveland, also noted that only 54% of children who had records indicating an ASD met CDC criteria for a diagnosis)
The American Academy of Paediatrics has recommended that all children be screened for autism spectrum disorders when they are 18 and 24 months old. This is "especially important, as early recognition and treatment improves outcomes," (Shlomo Shinnar, MD, PhD, of Albert Einstein College of Medicine in New York)
The difficulty for parents and medical practitioners is then to decide the optimum course of treatment from all of those alternative autism treatments that are available, with the best possible outcome for each individual child. Autism spectrum disorders can be divided into categories, low-functioning autism (IQ below 70), high-functioning autism (IQ above 70), and Aspergers syndrome (akin to high-functioning autism but with no language deficit).
Hypotheses For The Development Of Autism
In 2007 the National Institutes of Health announced an Autism Centers of Excellence (ACE) research program to investigate the causes of autism and identify new autism treatments. Initial research is focusing on genetic factors, brain imaging, brain chemicals e.g. neurotransmitters and functions, effect of early parent-child behaviour on autism, and learning in autistic children.
However, there is an increasing consensus among researchers that autism does not have a single cause, but is instead a complex disorder with a set of core aspects that have separate distinct causes. In other words, completely different underlying brain dysfunctions have been thought to result in the many autism symptoms, just as completely different brain problems result in mental retardation.
Chronic inflammatory process. There is considerable evidence from direct observation at autopsy and SPECT scanning of autistic brains that inflammation and resulting hypoperfusion (low oxygenated blood flow) are present in all cases of Autism. The positive benefits observed after hyperbaric oxygen treatments as well as supplying dietary vitamins and Omega 3 & 6 fatty acids with anti-inflammatory properties lend weight to support this hypothesis.
Infective agents or toxic chemicals exposure to infective agents or toxic chemicals are widely suggested but there is to date a lack of convincing evidence e.g. only a small percentage of autistic children show high levels of Mercury or other heavy metals which could be responsible for oxidative stress in the brain.
This may just be a consequence of the low blood & Cerebrospinal fluid flows in the brain allowing a build up in metal ion concentration. There is evidence for infective agents being present in some cases and may be responsible for triggering the widespread inflammatory response that reduces vital blood flows and oxygen to the developing brain cells.
Opioid hypothesis Gluten & Casein intolerance due to leaky gut syndrome. Evidence suggests a large percentage of Autistic children do show improvements in behaviour when Gluten & Casein are removed from their diet.
Reactions to childhood vaccinations or Thiomersal have effectively been ruled out as causal agents for Autism.
Definitions And Common Features In The Brains of Autistic Children
Pathophysiologyy
Autistic people tend to use different areas of the brain (yellow) for a movement task compared to a control group (blue).
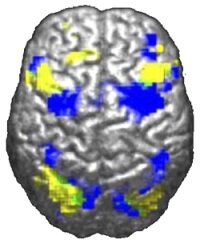
Powell K (2004) Opening a Window to the Autistic Brain
Autism affects the amygdale, cerebellum and many other parts of the brain. Unlike many other brain disorders such as Parkinson's, autism does not have a clear unifying mechanism at either the molecular, cellular, or systems level; it is not known whether autism is a few disorders caused by mutations converging on a few common molecular pathways, or is (like intellectual disability) a large set of disorders with diverse mechanisms.
Autism occurs because of a failure of the brain to develop in a way that allows the child to interact as we would expect. Autistic boys outnumber girls by approximately 4.5:1 and most have the 46,XY karyotype (i.e. the karyotype of healthy boys) suggesting that the condition has a genetic component.
One commonly suggested hypothesis that would explain the swelling of certain areas of the Autistic brain is the chronic inflammation in the cells and blood vessels supplying oxygen to the brain cells, leading to hypoxia which in turn causes a lack of connectivity of the brain cells and a failure to develop.
Abnormalities in affiliative behaviours of other species, which are associated with dysfunction of serotonin and the neuropeptides, oxytocin, and vasopressin, suggest that there may be a neurophysiological dysfunction involving one or more of these substances in autism in humans. i.e. in animal models, where there is a failure of an individual to bond with the family group there is a dysfunction associated with neurotransmitters within the brain.
Many independent single photon emission computed tomography (SPECT) and positron emission tomography (PET) research studies have revealed hypoperfusion (restricted blood flow or ischemia) in several areas of the autistic brain, most notably the temporal regions and areas specifically related to language comprehension and auditory processing.
Several studies show that diminished blood flow to these areas correlates with many of the clinical features associated with autism including repetitive, self-stimulatory and stereotypical behaviours, and impairments in communication, sensory perception, and social interaction.
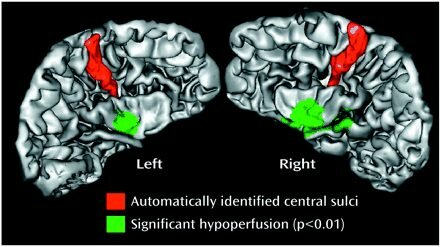
Temporal Lobe Dysfunction in Childhood Autism: A PET Study Monica Zilbovicius
These imaging and anatomic studies also reveal abnormalities in the cells in several regions of the brain, including the frontal and temporal lobes and the cerebellum. Enlargements of the amygdale and the hippocampus are common in childhood. Findings do however vary in each person. Hughes (2007) has observed the presence of underconnectivity in the brains of children with autism and related conditions.
This evidence suggests that hypoperfusion and resulting hypoxia is intimately associated with autism; however the next important questions are whether this is one of the causes of the problem and whether treatment to deal with this hypoxia can positively benefit autism.
In autism the associated hypoxia is not predominantly apoptotic (causing programmed cell death) or immediately fatal to brain neurons but associated with diminished functionality i.e. the brain cells are starved of Oxygen causing significant stress but not to the extent of killing them. Hypoperfusion (low blood flow) may contribute to defects not only by inducing hypoxia but allows abnormal metabolite or neurotransmitter accumulation as the reduced blood or Cerebrospinal Fluid flows fail to remove them.
Autism Treatments And Their Rationales - the R&D Gold Standard or Best Treatments Based Upon The Balance Of Probabilities
The interventions that are discussed are split into Primary autism treatments that are designed to deal with the root causes of Autism and Secondary autism treatments that deal with the symptoms. My recommendations are that parents endeavour to understand these differences and negotiate with their health care providers to obtain the best practicable range of therapies for their children at the earliest possible time.
Primary Autism Treatments In Priority Order
- Education. Effective treatment of associated behavioural problems includes intensive behavioural, educational, and psychological components. Interventions initiated at the time of diagnosis increase the likelihood of seeing a significant improvement in symptoms and behaviour. Regular screening of infants and toddlers for symptoms and signs of autistic disorder is crucial because it allows for early referral of patients for further evaluation and treatment. Such intense educational behavioural training with a high expectation of success and enthusiasm being transmitted to the child is crucial to improvements in behaviour
-
Hyperbaric Oxygen Therapy (HBOT) is based upon the Inflammatory Hypothesis for the causes of Autism and offers the best opportunity for treating the ongoing cause of the problem, hypoxia and subsequent inflammation of key areas of the brain. Increasing the amount of oxygen available to those areas of the brain that have failed to develop due to this lack of perfusion by oxygenated blood has been shown to increase the metabolic rate of brain cells stimulating their development and enhancing connectivity in those areas.
It also has the significant additional benefit of stimulating the patients own production of stem cells six-fold (CD-34) which are intimately involved in new blood vessel growth (angiogenesis) and the promotion of healing. Growth of new blood vessels in the brain is of critical importance as such improvements are believed to be permanent. There is not yet full agreement within the scientific community that inflammation or lack of oxygen cause autism but there is increasing evidence that individuals with traumatic brain injury (TBI) benefit quite dramatically from HBOT.
Cells need oxygen to fuel metabolism for cellular growth and repair. Healthy brains produce their own energy to maintain brain tissue and keep the rest of the body doing what it's supposed to do. That includes automatic processes like breathing and circulation, voluntary actions like walking and talking, as well as complex processing of auditory inputs and interpreting visual signals. In addition, should the brain swell inside the skull due to widespread inflammation that may increase the degree of hypoperfusion.
Johns Hopkins researchers have stated that because the inflammation process in the brain is associated with ongoing, chronic central nervous system dysfunctions, treatments of Autism should concentrate upon control of its detrimental effects. (Dr Vargas et al 2005) "There's a direct correlation between clinical outcome (in TBI) and the degree to which the brain's metabolism is restored," (Gaylan Rockswold, MD).
"In previous research we learned that the brain's energy production is improved and maintained with hyperbaric oxygen treatment, but this study confirms that hyperbaric oxygen treatment has a major impact in terms of increased energy production." Some if not all autistic children have inflammation around blood vessels in the brain that impedes blood flow. "
The decreased blood flow is correlated to how severe the autism is; the lower the blood flow to the brain, the worse the autism is," he said. "Hyperbaric oxygen therapy decreases inflammation and improves oxygen supply to the brain." (Dr. Rossignol) Despite the lack of Gold Standard scientific evidence for HBOT as a treatment for autism, anecdotal evidence and word-of-mouth have made this an increasingly important option to parents of children with autism.
By analogy with the growing body of evidence that Hyperbaric Oxygen Treatment can restore damaged or dormant brain cells in patients with Traumatic Brain Injury then this treatment must be viewed as the medical treatment most likely to result in significant improvements in behaviour & cognitative function in Autistic children. Care must be exercised however to use a treatment regime that produces a physiological effect and not a short term Pygmalion or Placebo effect that may be the result of mild hyperbaric treatment. -
Diet & Nutrition has a role in treatment and may help in certain cases using Omega 3 & Omega 6 fatty acid supplements, Vitamins B6, B12, thiamine, vitamin A and Gluten/Casein-Free Diets. The theory behind Gluten/Casein-free diets is based upon the opioid hypothesis of autism. In this hypothesis, defective intestinal enzymes (especially dipeptidyl-dipeptidase IV) allow large molecules to "leak" through the gut.
Gluten, and the structurally related Casein, are incompletely digested and pass through the gut as molecules with opioid-like properties. In larger doses, these molecules cause hallucinations. The effects of opioid-like compounds are, in part, the symptoms seen in autism, Asperger's, and other developmental disorders.
After one month of such a diet, challenging the child with a grilled cheese sandwich on whole wheat bread helps to determine if symptoms intensify after exposure to Gluten or Casein. Sensitive children become clearly worse after this meal. At least half of all autistic children are said to show improvements after starting a Gluten/Casein free diet. - Stem Cell Therapy is a potentially promising area - with foetal cord stem cells being injected into the patient showing stimulated brain development but much more research is necessary before it can be widely introduced.
Secondary Autism Treatments
- Chiropractic manipulation of the neck may help improve CNS fluid flow to the brain, helping to reduce levels of abnormal neurotransmitters present that inhibit brain cell communication.
- Pharmaceutical intervention is available but treats the symptoms rather than the root cause of the condition and many of the drugs used are known to have severe side effects. Children with autistic disorder appear sensitive to medication and may experience serious adverse effects that outweigh any beneficial effects. For example, children may develop catatonia when treated with haloperidol and other traditional neuroleptics. Drug therapy is ineffective in treating the core deficits of autism but may be effective in treating associated behavioural problems and comorbid disorders (a medical condition existing simultaneously but independently with autism).
- Although serotonin mimicking drugs and opioid antagonists, including naltrexone are reportedly beneficial, no pharmacologic agent is effective in the treatment of the core behavioural manifestations of autistic disorder. The possible benefits from drug therapy must be balanced against the likely adverse effects on a case-by-case basis.
Questionable Medicines & Autism Treatments
- Home oxygen chambers that offer mild hyperbaric oxygen treatment should be viewed with a degree of scepticism as trials using oxygen concentrators and a low pressure of 1.3 bar ATA using only air slightly enriched with Oxygen could not be replicated at other centres. Hyperbaric Oxygen treatment must use 100% oxygen and pressures of at least 1.5 Bar ATA to achieve a physiological response in the brain.
- Secretin has been shown to be ineffectual as a medication in treating Autism as six controlled clinical trials of secretin have demonstrated no effect. Certain findings suggest that Melatonin may have some beneficial effects.
- The use of anti-inflammatory drugs such as corticosteroids (Prednisolone), Minocycline, and non-steroidal anti inflammatories all have potentially serious side-effects or are even contra-indicated due to serious complications such as Reyes syndrome which worsen blood flow to the brain.
- Chelation therapy to remove heavy metals, although it has its proponents, is associated with significant health risks for what are unquantifiable benefits.
Autism Treatments - Conclusions And Recommendations
In reviewing the available research literature it can be concluded that there is a growing body of evidence to show that injured brains or those of children that have failed to develop as expected may be stimulated into an enhanced metabolic state and allow the bodys own systems to carry out repairs by interventions that are known to do no harm but have the potential to improve significantly those cognitative skills, social understanding and interactions that are lacking in those with Autism.
The medical profession and those of us involved in offering autism treatments owe a duty of care to all autistic children and their families and to offer the best practical advice about therapies that are believed to improve the childs condition without exposing them to excessive risks. This unequivocal advice is to take concerted actions as soon as a child is diagnosed with any of the conditions within the autistic spectrum disorder.
- Enrol the child in an intensive educational therapy program commensurate with the childs diagnosis at the earliest possible time.
- Negotiate with health care providers to treat the child using hyperbaric oxygen therapy using 100% Oxygen at a minimum of 1.5 Bar ATA for approximately 40 treatment sessions or until no further improvement in cognitative behaviour occurs. Do not be tempted to invest in a Mild hyperbaric chamber and Oxygen concentrator. There is no substitute for an approved and medically supervised chamber.
- Evaluate the efficacy of Casein/Gluten-Free Diet as well as supplementing the diet with the correct doses of Vitamins A, B6 & B12 and Omega 3 & Omega 6 fatty acids under the guidance of a dietician. Many autistic children with leaky guts may build up opiate like by-products in their blood streams that will exacerbate existing symptoms.
- Monitor the childs progress and accept the prescription by your doctor of appropriate drugs when there is an overwhelming requirement.

Return from the Autism Treatments Rationale discussion to the Home Page
Learn more about Characteristics For Autism Spectrum Disorders, Autism And Vaccinations, Autism Types, Early Symptoms of Autism...











